


UZEDY is a long-acting injectable (LAI) risperidone treatment designed for adults with schizophrenia that utilizes the innovative drug delivery platform SteadyTeq™.1,2 The safety of UZEDY for patients with schizophrenia is based on adequate and well-controlled studies of oral risperidone, and the efficacy and safety of UZEDY was established in the phase 3 clinical trial, Risperidone Subcutaneous Extended-release (RISE).1,2
The SteadyTeq™ platform enables each dose of UZEDY to generate a rapid absorption phase followed by a slower, secondary absorption phase over several weeks. UZEDY reaches therapeutic plasma concentrations within 6 to 24 hours of initiation and maintains clinically relevant plasma levels throughout the dosing interval.1,3 The net result is a streamlined initiation or reinitiation without the need for oral supplementation or loading doses.1,3 In addition to the pharmacokinetic features, the administration features of UZEDY result in an LAI that can be administered subcutaneously in the abdomen or back of the upper arm for all appropriate patients.1
UZEDY was evaluated in the double-blind, placebo-controlled, randomized relapse prevention study RISE, which compared UZEDY once monthly (Q1M) and once every 2 months (Q2M) with placebo in adult patients with schizophrenia.1,2,4 In RISE, patients receiving UZEDY Q1M demonstrated significant reduction in the risk of relapse by 80% compared with patients receiving placebo (Figure 1). In patients receiving UZEDY Q2M, the reduction in risk of relapse was 62.5% compared with placebo.2
Figure 1. Patients With Impending Relapse
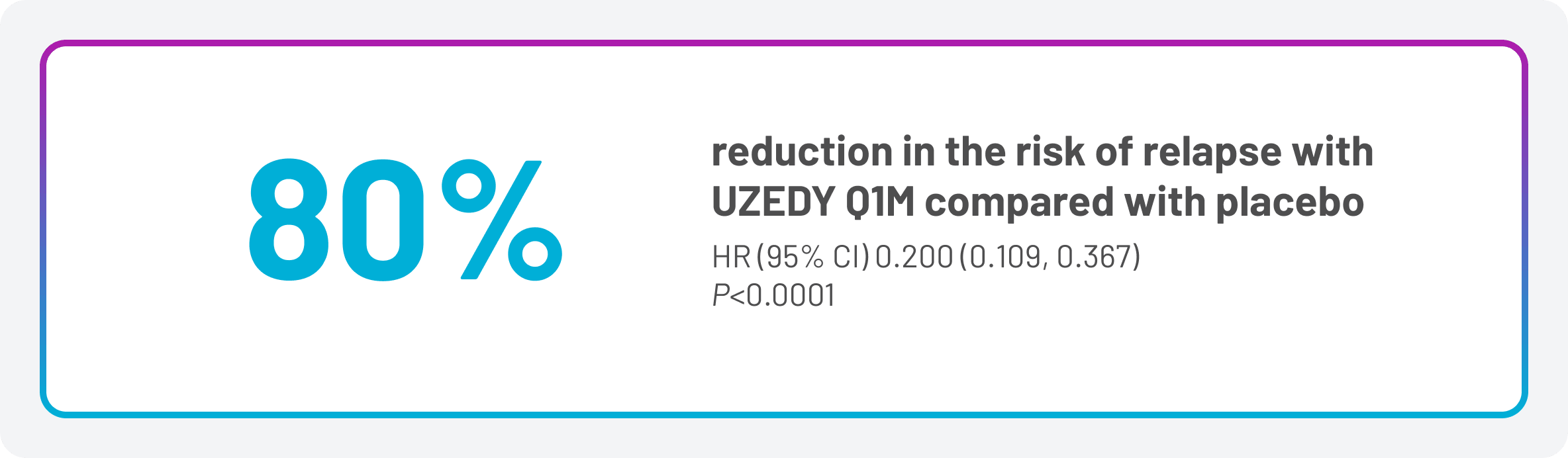
CI, confidence interval; HR, hazard ratio.
The safety profile of oral risperidone in adults with schizophrenia has been well characterized. The safety profile of UZEDY for patients with schizophrenia is based on adequate and well-controlled studies of oral risperidone, and the safety profile of UZEDY is expected to be similar to that of corresponding oral risperidone doses of 2 to 5 mg daily.1 Figure 2 lists the adverse reactions occurring in at least 2% of patients in the RISE trial.
Figure 2. Adverse Reactions Occurring in ≥2% of Patients
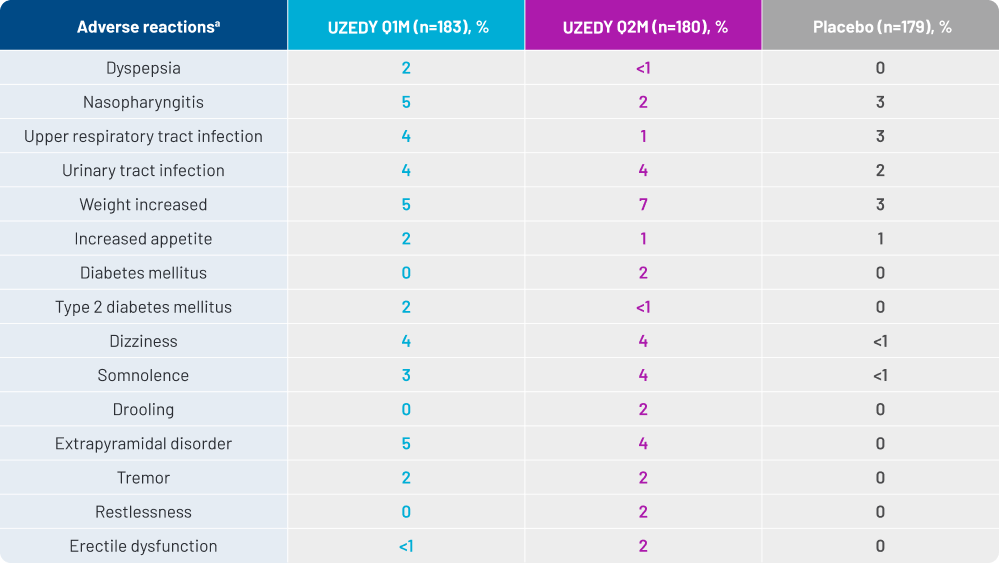
aThose occurring in ≥2% of patients treated with UZEDY and with higher frequency than in patients receiving placebo.
A retrospective claims data analysis was conducted to investigate the demographic, clinical, and treatment characteristics of eligible adult patients in the United States who had received a prescription for UZEDY. The analysis utilized retrospective claims data from the EVERSANA database, covering August 2018 to February 2024. This database accounts for 90% of all prescriptions in the US.5 While the information that this database provides on the use of UZEDY is useful, it is important to note that no conclusions of safety or efficacy can be made of a retrospective administrative claims data analysis.
Patients included in the study were those prescribed UZEDY between May 2023 and February 2024, with either at least 2 months of data prior to the start of the analysis period or a first claim date prior to May 1, 2023. In this analysis, UZEDY Q1M and UZEDY Q2M were treated as separate medications, with 25 patients common to both groups. Patient data were analyzed starting at the latter of either the first claim date for UZEDY or the first claim for a schizophrenia diagnosis.5
Figure 3. Real-World Persistence Among Patients With Schizophrenia Treated With UZEDY
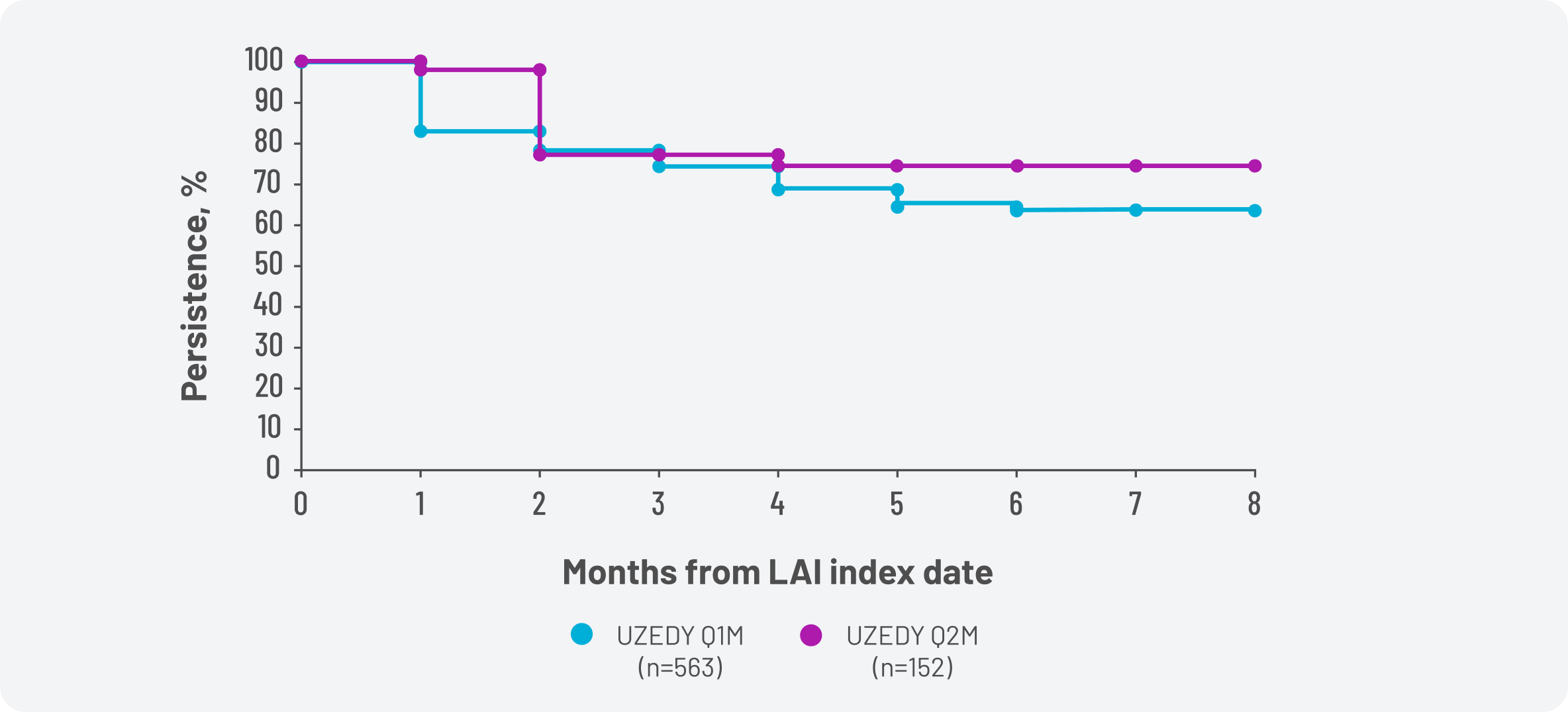
Persistence of treatment was assessed using the Kaplan-Meier methodology, which calculates persistence based on the time to treatment discontinuation. Subjects who exceeded 30 days between the end of 1 prescription and the start of the next—indicating the end of the treatment's allotted supply—were discontinued. Approximately 74% of adult patients with schizophrenia prescribed UZEDY were persistent with their treatment 4 months after receiving their first prescription (Figure 3).5
The retrospective claims data were additionally utilized to evaluate adherence among adult patients with schizophrenia who were treated with UZEDY Q1M and UZEDY Q2M. For the adherence analysis, patients were deemed adherent if their antipsychotic medication covered at least 80% of the days analyzed for that patient.5
Figure 4. Adherence Among Patients With Schizophrenia Treated With UZEDY
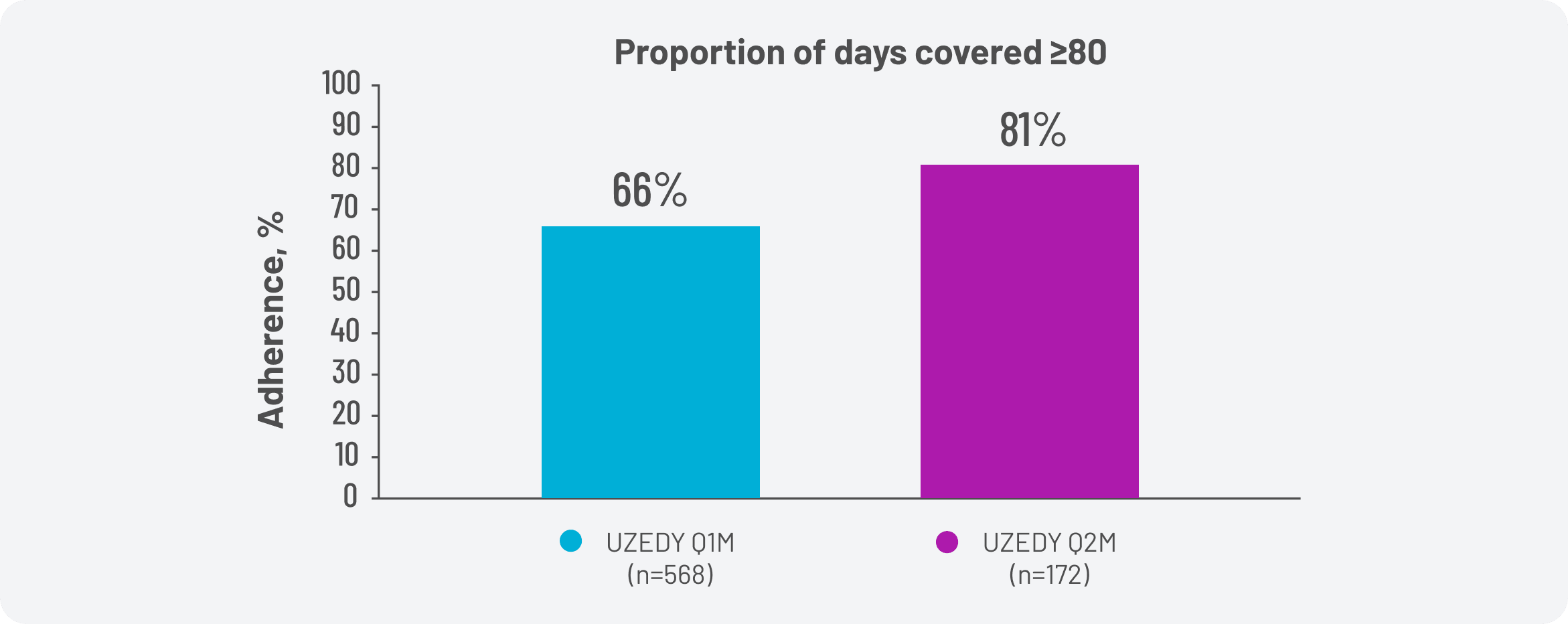
Patients were observed for 1 year; for the number of days between the beginning of the analysis and the date of the patient's last recorded activity; or for the number of days from the beginning of the analysis to the date the patient switched to another LAI—whichever period was shortest. Among adult patients with schizophrenia treated with UZEDY, 66% of those taking UZEDY Q1M were adherent to their treatment, and 81% of those taking UZEDY Q2M were adherent (Figure 4).5
Additional post hoc and exploratory analyses were conducted in the RISE clinical trial. As with the data above, it is important to remember that, due to the exploratory and post hoc nature of these analyses, no determination of statistical significance can be made, and conclusions should not be drawn from these findings.
The patient-reported Schizophrenia Quality of Life Scale (SQLS) is a 33-item scale divided into 2 domains: “psychosocial feelings” and “cognition and vitality”, with a decrease in scores signifying an increase in quality of life. Patients with schizophrenia treated with UZEDY Q1M and Q2M exhibited a decrease in SQLS scores from baseline. In contrast, scores increased for patients in the placebo group (Figure 5A).6
Additionally, the European Quality of Life 5-Dimension 5-Level Visual Analog Scale (EQ-5D-5L VAS) is a 2-part questionnaire used to assess health-related quality of life, with higher scores indicating better quality of life. In part 1, patients evaluate their health state across 5 dimensions—mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. In part 2, patients rate their overall health state. Patients with schizophrenia in the UZEDY Q1M and Q2M groups showed increases in EQ-5D-5L VAS scores from baseline, while scores decreased for those in the placebo group (Figure 5B).6
Figure 5. RISE Exploratory Analysis: Patient-Centered Outcomes
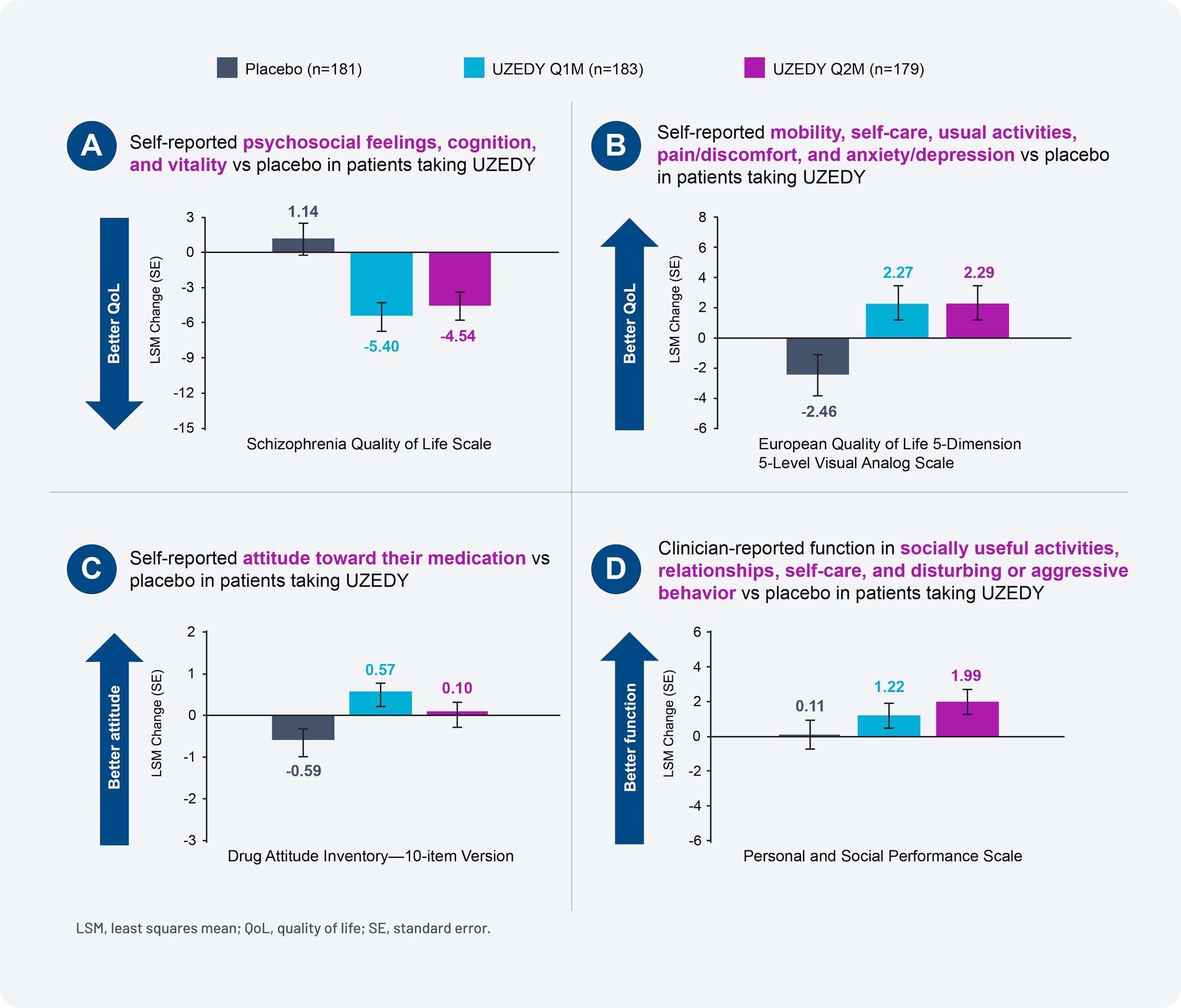
The patient-reported Drug Attitude Inventory–10-Item Version (DAI-10) covers 3 domains: subjective positive, subjective negative, and attitude toward medication. A positive patient score on the DAI-10 reflects a favorable attitude toward psychiatric medication. Patients with schizophrenia treated with UZEDY Q1M and Q2M exhibited an increase in DAI-10 scores from baseline to the end of treatment, whereas scores decreased for those in the placebo group (Figure 5C).6
Finally, the clinician-reported Personal and Social Performance (PSP) scale measures patient functioning across 4 categories: socially useful activities (housework, work, or study), personal and social relationships (with partners, family, or friends), self-care (personal hygiene and appearance), and disturbing and aggressive behaviors. Lower scores indicate functioning requiring intensive supervision, while higher scores reflect better personal and social functioning. Patients in the UZEDY Q1M and Q2M groups demonstrated numerical improvements in PSP scores from baseline compared with those in the placebo group (Figure 5D).6
UZEDY offers a variety of features that clinicians and patients may consider as part of a comprehensive discussion of schizophrenia treatment (Figure 6). In addition to the clinical data reviewed above, the pharmacokinetic (PK) profile of UZEDY results in rapid attainment of therapeutic plasma levels in 6 to 24 hours that are sustained for the duration of the dosing interval.1,2 Initiation of UZEDY is streamlined, with a single-dose initiation or reinitiation without the need for loading doses or oral supplementation.1
Figure 6. Factors to Consider When Choosing UZEDY for Patients With Schizophrenia
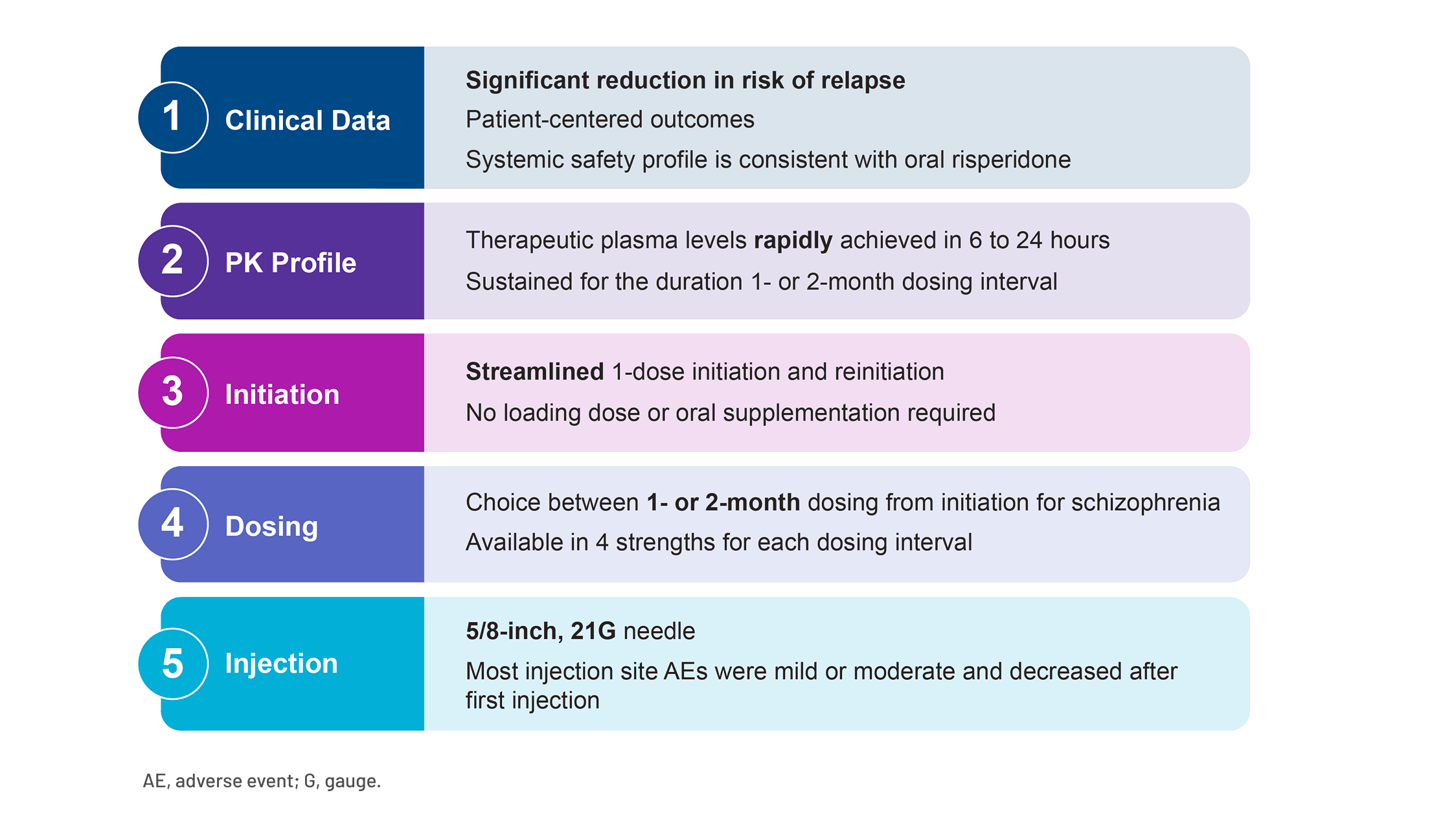
The dosing of UZEDY can be tailored to the needs of the patient, with the choice between 1- or 2-month dosing and 4 available strengths for each dosing interval for patients with schizophrenia.1 Additionally, UZEDY is available in a prefilled syringe with a 5/8-inch, 21G needle that can be administered subcutaneously in the back of the upper arm or abdomen.1 In the RISE study, injection site reactions (ISRs) were mild or moderate and, overall, ISRs decreased in frequency after the first injection.7,8 The most common ISRs with UZEDY in patients with schizophrenia (≥5% and greater than placebo) were pruritus and nodule.1
- In the RISE clinical trial, adult patients receiving UZEDY Q1M demonstrated significantly reduced risk of relapse by 80% compared with patients receiving placebo2
- The safety profile of UZEDY for patients with schizophrenia is based on adequate and well-controlled studies of oral risperidone, and the safety profile of UZEDY is expected to be similar to that of corresponding oral risperidone doses of 2 to 5 mg daily1
- In a retrospective administrative claims data analysis, approximately 74% of adult patients with schizophrenia prescribed UZEDY were persistent with their treatment 4 months after receiving their first prescription.5 These data also demonstrated that 66% of those taking UZEDY Q1M were adherent to their treatment, and 81% of those taking UZEDY Q2M were adherent5
- Additional post hoc and exploratory analyses were conducted from the RISE clinical trial that assessed patient-centered outcomes; however, due to the exploratory and post hoc nature of these analyses, no determination of statistical significance can be made, and conclusions should not be drawn from these findings
- UZEDY offers a variety of features that clinicians and patients may consider as part of a comprehensive discussion of schizophrenia treatment
- UZEDY® (risperidone) extended-release injectable suspension Current Prescribing Information. Parsippany, NJ: Teva Neuroscience, Inc.
- Kane JM, Harary E, Eshet R, et al. Efficacy and safety of TV-46000, a long-acting, subcutaneous, injectable formulation of risperidone, for schizophrenia: a randomised clinical trial in the USA and Bulgaria. Lancet Psychiatry. 2023;10(12):934-943.
- Merenlender Wagner A, Elgart A, Perlstein I, et al. Phase 1 open-label study assessing the pharmacokinetics and safety of TV-46000, a novel long-acting subcutaneous injectable formulation of risperidone. Presented at: European Congress of Neuropathology; October 2-5, 2021; Lisbon, Portugal. Poster P.0463.
- Data on file. Parsippany, NJ: Teva Neuroscience, Inc.
- Thompson S, Nathan R, Suett M, et al. Real-world TV-46000 prescribing behaviors in the United States since approval to treat adults with schizophrenia: United States claims database analysis of treatment patterns. Presented at: Academy of Managed Care Pharmacy (AMCP) Nexus 2024; October 14-17, 2024; Las Vegas, NV.
- Citrome L, Suett M, Franzenburg KR, et al. TV-46000, a long-acting subcutaneous antipsychotic agent, demonstrated improved patient-centered outcomes in patients with schizophrenia. Neuropsychiatr Dis Treat. 2024;20:1901-1917.
- Correll CU, Kane JM, Suett M, et al. Efficacy and safety of TV-46000, subcutaneous long-acting risperidone, by injection site (upper arm/abdomen): post hoc analysis of the RISE study. Presented at: Psych Congress; October 29–November 1, 2021; San Antonio, TX.
- Correll CU, Kane JM, Suett M, et al. TV-46000–A long-acting subcutaneous antipsychotic (LASCA) for the treatment of schizophrenia: local tolerability and injection site reactions. Presented at: Psych Congress; September 6-10, 2023; Nashville, TN.