


The clinical course of schizophrenia is often characterized by recurrent relapse.1,2 Many of the consequences of relapse, which range from treatment resistance to arrests and homelessness, may begin after the first relapse.3-5 For this reason, early intervention and taking steps to delay relapse is important for patients with schizophrenia.6
Long-acting injectables (LAIs) provide extended dosing intervals with fewer opportunities to miss a dose, and the expectation of sustained, stable therapeutic levels of antipsychotic after receiving an injection.7,8 The American Psychiatric Association guidelines and experts recommend LAIs for any patient for whom long-term antipsychotic therapy is indicated, and should be introduced early and often, as part of a comprehensive discussion of treatment options.7-12 Despite this, LAIs are often reserved as a last resort for patients or not offered by clinicians due to the perception that the patient will not accept an LAI or past rejection of LAIs.13,14
In reality, studies suggest that patients may consider LAIs, after learning about their advantages and disadvantages, and some patients may prefer this option.15-17 Patients may not accept an LAI the first time, so it is important to introduce LAIs early to the treatment conversation and revisit them on a regular basis as appropriate. Consistent dialogue and communication strategies such as motivational interviewing may encourage patients to reconsider the potential benefits of an LAI even if they have rejected the option before.18,19
There are a number of LAIs currently available for schizophrenia treatment, each with different pharmacokinetic, administration, and usage attributes that may impact clinical decision making.20-24 UZEDY is a different kind of LAI for adults with schizophrenia that utilizes the innovative drug delivery platform SteadyTeqTM to offer a range of features that clinicians and patients may want to consider when selecting an LAI.25,26
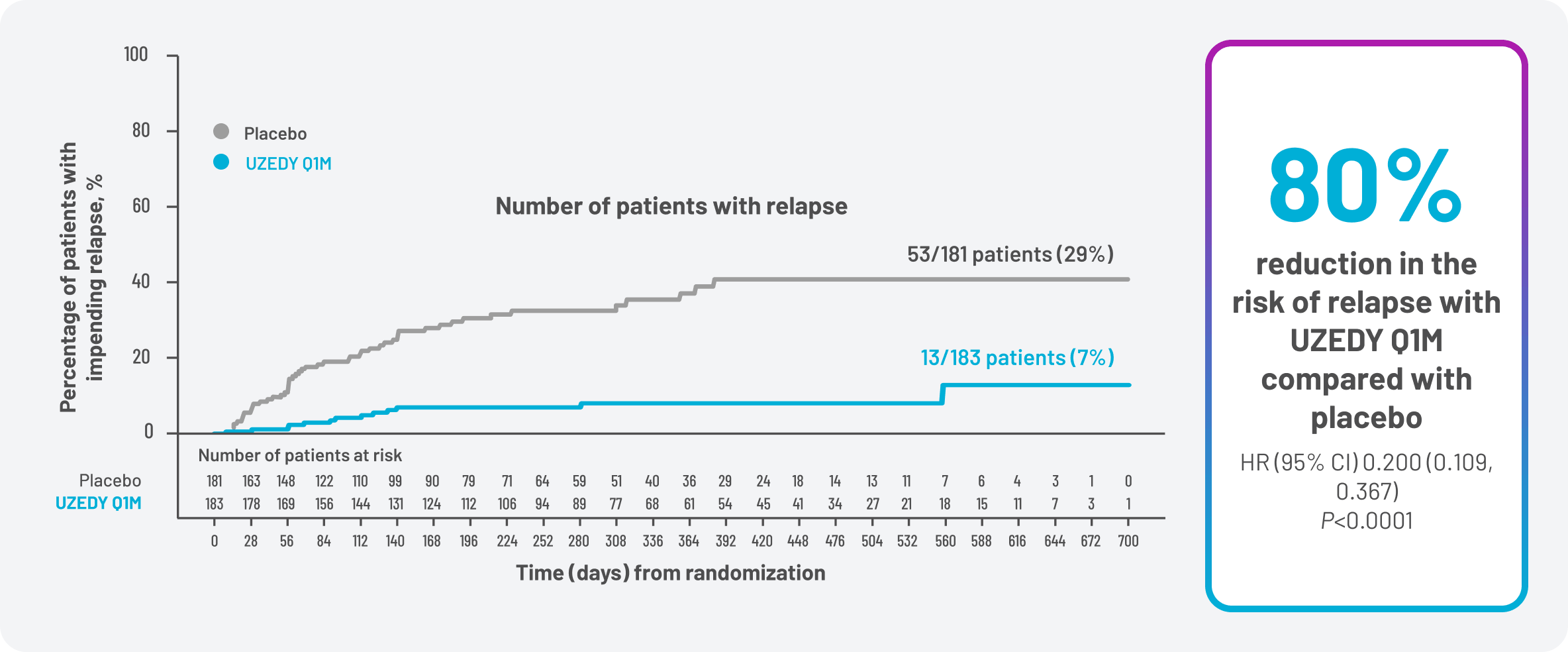
UZEDY was evaluated in the double-blind, placebo-controlled, randomized relapse prevention study RISE, which compared UZEDY once monthly (Q1M) and once every 2 months (Q2M) with placebo in patients with schizophrenia.25-27 In RISE, patients receiving UZEDY Q1M demonstrated a significantly reduced risk of relapse by 80% compared with patients receiving placebo (Figure 1).25 In patients receiving UZEDY Q2M, the reduction in risk of relapse was 62.5% compared with placebo.25
Figure 1. Patients With Impending Relapse
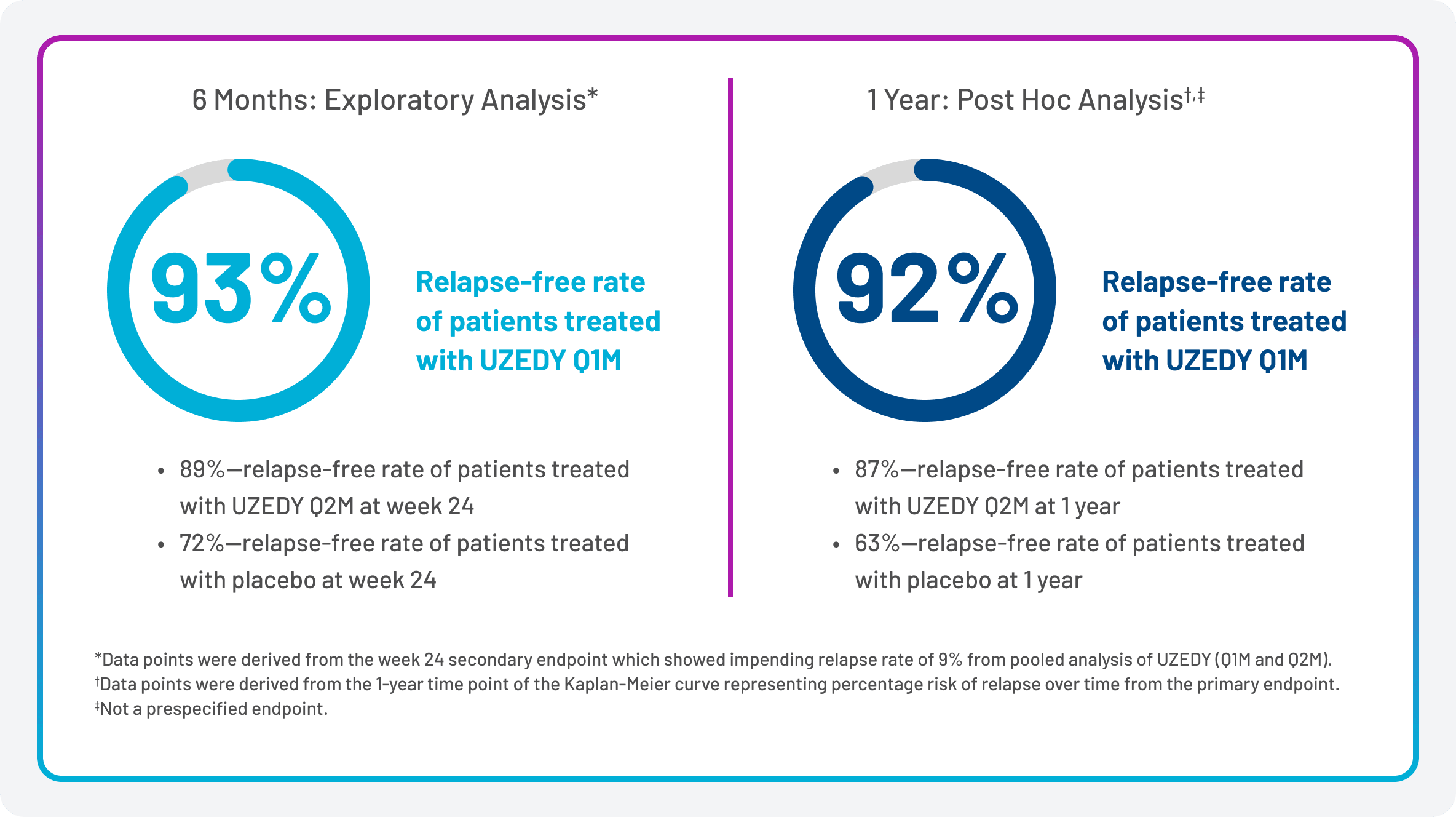
Exploratory and post hoc analyses of these studies were conducted at 6 months and 1 year. At week 24, the relapse-free rate for patients receiving UZEDY Q1M was 93%, while it was 89% for those receiving UZEDY Q2M, compared with 72% in the placebo group.27 At the one-year mark, the relapse-free rates for the UZEDY Q1M and Q2M groups were 92% and 87%, respectively, compared with 63% for the placebo group (Figure 2).27 It is important to remember that, due to the exploratory and post hoc nature of these analyses, no determination of statistical significance can be made, and conclusions should not be drawn from these findings.
Figure 2. Relapse-Free Rate of Patients at 6 Months and 1 Year
The safety profile of UZEDY for patients with schizophrenia is based on adequate and well-controlled studies of oral risperidone, which has been well characterized, and is expected to be similar to that of corresponding oral risperidone doses of 2 to 5 mg daily.26
The most common adverse reactions with oral risperidone (≥5% and greater than placebo) were parkinsonism, akathisia, dystonia, tremor, sedation, dizziness, anxiety, blurred vision, nausea, vomiting, upper abdominal pain, stomach discomfort, dyspepsia, diarrhea, salivary hypersecretion, constipation, dry mouth, increased appetite, increased weight, fatigue, rash, nasal congestion, upper respiratory tract infection, nasopharyngitis, and pharyngolaryngeal pain.26
In addition to efficacy and safety, there are several important factors for clinicians and patients to consider when selecting an LAI. Key considerations may include patient preferences for features such as dosing interval or needle size and clinician discretion regarding administration and pharmacokinetic features.
Table 1 includes a list of features of some LAIs available for schizophrenia treatment.20-24,26 Although this information should not be construed to imply any difference in safety, efficacy, or clinical outcomes, these features may be considered as part of a larger discussion about treatment options.
Table 1. Pharmacokinetic, Administration, and Usage Attributes of LAIs
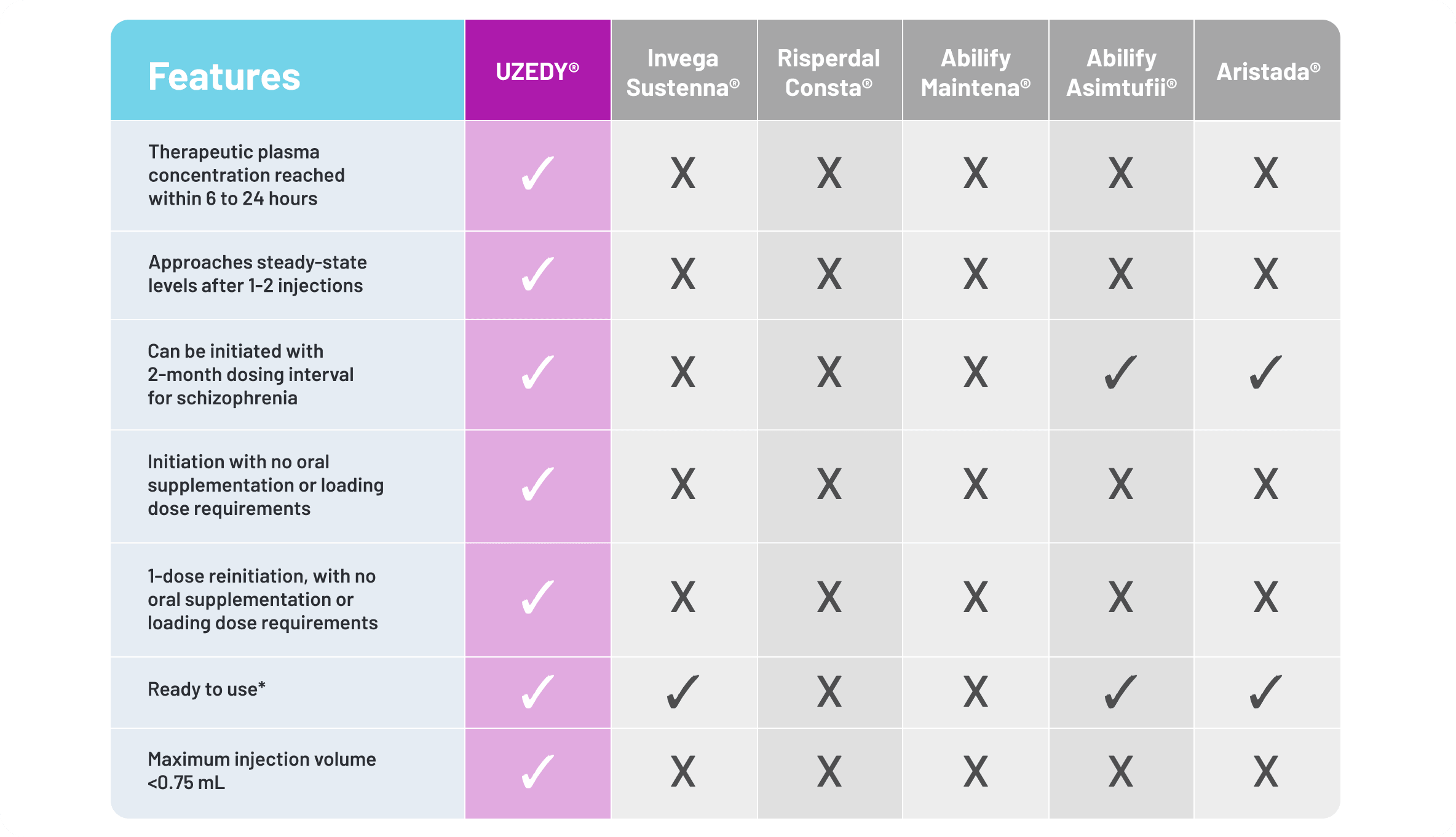
*No reconstitution or premixing required.
Only UZEDY offers a pharmacokinetic profile that attains therapeutic plasma concentrations within 6 to 24 hours of administration. The net result is that UZEDY maintained clinically relevant plasma levels throughout the dosing interval, and steady-state levels of risperidone and its metabolite, 9-hydroxyrisperidone, were approached within 2 months of initiation of UZEDY.26
The dosing interval and dosage strength of UZEDY can be tailored to the individual needs of patients with schizophrenia.26 UZEDY may be a suitable option for patients who don't want to take a daily pill or prefer less frequent dosing, as it is available in 1- or 2-month dosing for schizophrenia.26 UZEDY also does not require oral supplementation or loading doses when initiating treatment.26 This feature streamlines the treatment initiation process and offers a single-injection reinitiation protocol for patients who miss their regularly scheduled dose.26
In a companion survey involving 63 patients, 24 physicians, and 25 nurses assessing perceptions regarding the ease of use and satisfaction with UZEDY, 90% of patients with schizophrenia surveyed indicated a preference for continuing UZEDY over their prior schizophrenia medications.28
- Despite the potential consequences of schizophrenia relapse, LAIs are often underutilized by clinicians or reserved as a last resort; however, consistent dialogue and patient education may encourage patients to consider an LAI1,2,13-18
- UZEDY significantly reduced the risk of relapse when compared with placebo, with an 80% reduction for Q1M dosing25
- The safety profile of UZEDY is expected to be similar to that of oral risperidone26
- UZEDY offers a variety of pharmacokinetic, administration, and usage features, including streamlined initiation and reinitiation, availability of 1- or 2-month dosing for schizophrenia, and achievement of therapeutic plasma concentrations within 6 to 24 hours of administration26
- Kane JM, Correll CU. Optimizing treatment choices to improve adherence and outcomes in schizophrenia. J Clin Psychiatry. 2019;80(5):IN18031AH1C.
- Alvarez-Jiminez M, Priede A, Hetrick SE, et al. Risk factors for relapse following treatment for first episode psychosis: a systematic review and meta-analysis of longitudinal studies. Schizophr Res. 2012;139(1-3):116-128.
- Nasrallah HA. 10 devastating consequences of psychotic relapses. Curr Psychiatry. 2021;20(5):9-12.
- Emsley R, Oosthuizen P, Koen L, et al. Comparison of treatment response in second-episode versus first-episode schizophrenia. J Clin Psychopharmacol. 2013;33(1):80-83.
- Takeuchi H, Siu C, Remington G, et al. Does relapse contribute to treatment resistance? Antipsychotic response in first- vs. second-episode schizophrenia. Neuropsychopharmacology. 2019;44(6):1036-1042.
- Girardi P, Del Casale A, Rapinesi C, et al. Predictive factors of overall functioning improvement in patients with chronic schizophrenia and schizoaffective disorder treated with paliperidone palmitate and aripiprazole monohydrate. Hum Psychopharmacol. 2018;33(3):e2658.
- American Psychiatric Association. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia. 3rd ed. Washington, DC: American Psychiatric Association; 2021.
- Bera RB. Patient outcomes within schizophrenia treatment: a look at the role of long-acting injectable antipsychotics. J Clin Psychiatry. 2014:75(suppl 2):30-33.
- Correll CU, Martin A, Patel C, et al. Systematic literature review of schizophrenia clinical practice guidelines on acute and maintenance management with antipsychotics. Schizophrenia (Heidelb). 2022;8(1):5.
- American Association of Community Psychiatrists. Clinical Tip Series. Long Acting Antipsychotic Medications. Accessed February 23, 2026. https://issuu.com/gaparticles/docs/aacp_clinical_tip-laa_december_2017_/1
- Gardner KN, Nasrallah HA. Managing first-episode psychosis: rationale and evidence for nonstandard first-line treatments for schizophrenia. Curr Psychiatry. 2015;14(7):33-45.
- Kane JM, Agid O, Castle DJ, et al. The use of long-acting injectables for people with schizophrenia: consensus panel recommendations for overcoming barriers and implementing treatment. Neurol Ther. 2025;14(6):2551-2581.
- Weiden PJ, Roma RS, Velligan DI, et al. The challenge of offering long-acting antipsychotic therapies: a preliminary discourse analysis of psychiatrist recommendations for injectable therapy to patients with schizophrenia. J Clin Psychiatry. 2015;76(6):684-690.
- Lindenmayer JP, Glick ID, Talreja H, Underriner M. Persistent barriers to the use of long-acting injectable antipsychotics for the treatment of schizophrenia. J Clin Psychopharmacol. 2020;40(4):346-349.
- Medrano S, Abdel-Baki A, Stip E, Potvin S. Three-year naturalistic study on early use of long-acting injectable antipsychotics in first episode psychosis. Psychopharmacol Bull. 2018;48(4):25-61.
- Blackwood C, Sanga P, Nuamah I, et al. Patients' preference for long-acting injectable versus oral antipsychotics in schizophrenia: results from the patient-reported medication preference questionnaire. Patient Prefer Adherence. 2020;14:1093-1102.
- Caroli F, Raymondet P, Izard I, et al. Opinions of French patients with schizophrenia regarding injectable medication. Patient Prefer Adherence. 2011;5:165-171.
- Franzenburg KR, Hansen RT, Suett M, et al. Perspectives of psychiatrists and psychiatric nonphysicians on treating schizophrenia with long-acting injectable antipsychotics: subgroup analysis from the multinational ADVANCE study. Presented at: Annual Psych Congress Elevate; May 28-31, 2025; Las Vegas, NV.
- Miller WR, Rollnick S, eds. Motivational Interviewing: Helping People Change. 4th ed. The Guilford Press; 2023.
- Invega Sustenna® (paliperidone palmitate). Prescribing Information. Titusville, NJ: Janssen Pharmaceuticals, Inc.
- Risperdal Consta® (risperidone). Prescribing Information. Titusville, NJ: Janssen Pharmaceuticals, Inc.
- Abilify Maintena® (aripiprazole). Prescribing Information. Otsuka America Pharmaceutical, Inc.
- Abilify Asimtufii® (aripiprazole). Prescribing Information. Otsuka Pharmaceutical, Inc.
- Aristada® (aripiprazole lauroxil). Prescribing Information. Alkermes, Inc.
- Kane JM, Harary E, Eshet R, et al. Efficacy and safety of TV-46000, a long-acting, subcutaneous, injectable formulation of risperidone, for schizophrenia: a randomised clinical trial in the USA and Bulgaria. Lancet Psychiatry. 2023;10(12):934-943.
- UZEDY® (risperidone) extended-release injectable suspension Current Prescribing Information. Parsippany, NJ: Teva Neuroscience, Inc.
- Data on file. Parsippany, NJ: Teva Neuroscience, Inc.
- Robinson DG, Suett M, Wilhelm A, et al. Patient and healthcare professional preferences for characteristics of long-acting injectable antipsychotic agents for the treatment of schizophrenia. Adv Ther. 2023;40(5):2249-2264.